"One Heart, Two Treatments": One-Stop K-Clip® Tricuspid Annuloplasty Combined with Left Atrial Appendage Closure Successfully Completed at Zhongnan Hospital of Wuhan University
In the field of structural heart disease, one-stop combined interventional procedures represent the future direction of development. Recently, a team led by Professor Zhang Gangcheng from the Structural Heart Disease Center of the Cardiovascular Hospital at Zhongnan Hospital of Wuhan University, in collaboration with teams led by Professor Liu Jinping (Cardiac Surgery), Professor Lu Zhibing (Cardiology), and Professor Wang Bin (Cardiovascular Ultrasound), successfully performed a one-stop minimally invasive procedure combining “K-Clip® Transcatheter Tricuspid Annuloplasty” with “Transcatheter Left Atrial Appendage Closure (LAAC)” on a complex patient presenting with both a high risk of stroke and symptomatic severe tricuspid regurgitation.
The success of this procedure not only resolved the patient’s two major chronic conditions in a single intervention, thereby avoiding the risks and suffering associated with multiple surgeries, but also demonstrated the outstanding capabilities of the Cardiovascular Hospital at Zhongnan Hospital in integrating multiple technologies and fostering team collaboration. It provides a new model for the comprehensive management of complex heart diseases.


Patient Profile
The patient is a 68-year-old female admitted due to "chest tightness and shortness of breath for 5 years." Five years ago, she began experiencing intermittent chest tightness and dyspnea after exertion, accompanied by bilateral lower limb edema and decreased physical stamina. Symptoms improved slightly with rest. She had no history of syncope, consciousness disorders, cough, or hemoptysis and had not received prior treatment.
Previous diagnoses at other hospitals indicated "Atrial Fibrillation (AF)" combined with "Valvular Heart Disease." She intermittently took "Rivaroxaban" but could not adhere to regular medication due to recurrent bleeding. Subsequently, she was treated long-term with "Spironolactone, Sacubitril/Valsartan Sodium, and Metoprolol Succinate," yet her dyspnea gradually worsened. Echocardiography at an outside hospital indicated "Severe Tricuspid Regurgitation." Upon admission, echocardiography revealed "Cardiomegaly, mild Mitral Regurgitation, and Extreme Tricuspid Regurgitation."
Core Patient Issues:
- Stroke Risk: Persistent atrial fibrillation with a CHA₂DS₂-VASc score of 4, placing her in a high-risk category for stroke. Additionally, she faced significant risks associated with long-term anticoagulation therapy.
- Heart Failure Symptoms: Echocardiography confirmed severe functional tricuspid regurgitation (TR), leading to secondary right heart failure. Symptoms included exertional chest tightness, dyspnea, bilateral lower limb edema, and reduced physical capacity. Despite medical, shortness of breath has continued to worsen gradually, with the emergence of paroxysmal nocturnal dyspnea and orthopnea, indicating poor drug efficacy.
Clinical Decision:The patient declined surgical intervention. Following multidisciplinary discussion and in-depth assessment, it was determined that a single interventional procedure addressing both issues simultaneously would provide the greatest benefit to the patient. Consequently, they decided to perform a one-stop "K-Clip® Tricuspid Annuloplasty + Left Atrial Appendage Closure (LAAC)" surgery, aiming to provide the most comprehensive protection with minimal trauma.
Pre-procedural Assessment
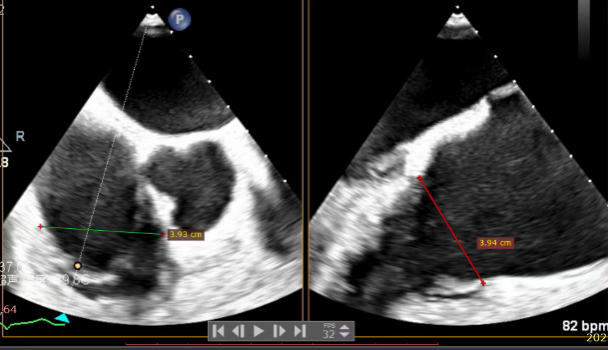
Echocardiographic Assessment: Echocardiography revealed left atrial enlargement. The left atrial appendage (LAA) orifice was 32mm with no thrombus inside. Tricuspid regurgitation was extreme (average vena contracta 18mm). Regurgitant jets were located at the anterior-septal, central, and posterior-septal commissures, with a central gap measuring approximately 13x5.9mm. The annulus was mildly dilated (average diameter 43mm). The tricuspid leaflets showed thickening and degenerative changes.
CTA Assessment: Showed a giant, wide-mouthed, conical "cauliflower-shaped" LAA. The right coronary artery (RCA) runs toward the atrial side, with a distance greater than 3mm between the RCA and the annulus during both systole and diastole.
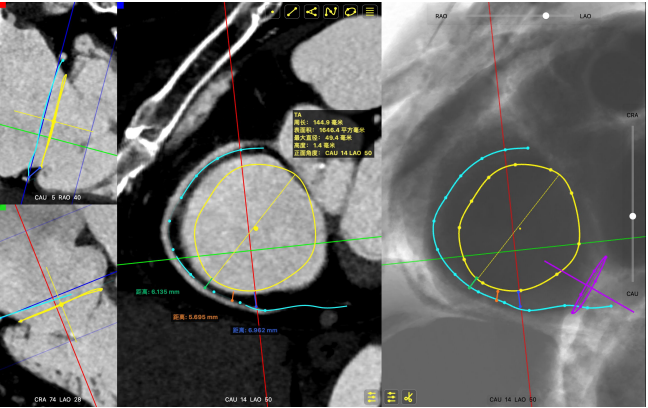
Systolic Tricuspid Annulus: Circumference 138mm, Area 1468mm².
Diastolic Tricuspid Annulus: Circumference 145mm, Area 1646mm².
Surgical Strategy
After multidimensional evaluation using pre-operative ultrasound and CT, Professor Zhang Gangcheng's team decided on a one-stop interventional approach: performing the LAAC first, followed by the tricuspid valve clipping and annuloplasty.
The plan involved implanting a 12T K-Clip® at the posterior-septal commissure (biased towards the posterior leaflet) and a 14T K-Clip® at the anterior-posterior commissure. This precise dual-point positioning strategy was designed to effectively reduce the tricuspid annulus diameter, improve leaflet coaptation, and directly correct tricuspid regurgitation at the anatomical level, providing critical structural support for post-operative recovery.
Procedure Details
The entire procedure was guided by both Transesophageal Echocardiography (TEE) and Digital Subtraction Angiography (DSA).
Left Atrial Appendage Closure (LAAC):The delivery system was successfully advanced into the left atrium. Precise measurements of the LAA orifice and depth were taken under multi-angle TEE and DSA guidance. Given the LAA's large orifice (nearly 34mm), conical cauliflower shape, and shallow usable depth, a LACBES2434 occluder was selected. Using the "extreme coin technique," the closure was successfully achieved.
DSA


K-Clip® Tricuspid Annuloplasty (Seamless Transition):Immediately after LAAC, the operators established a new vascular access route and advanced the K-Clip® delivery system directly into the right atrium, targeting the posterior-septal and anterior-posterior commissures of the tricuspid annulus. Under real-time ultrasound guidance, the team precisely anchored, clipped, and released the devices.
Immediate intraoperative echocardiographic verification showed that the tricuspid regurgitation area was significantly reduced from a preoperative grade of 5+(pre-op) to 2+(post-op), downgrading the severity from extreme to mild-moderate.
1.Baseline assessment of regurgitation severity.
2.Advancement of the steerable large sheath and delivery system under ultrasound guidance.
3.Steering and rotating the delivery system to target the site while engaging the anchor screw via the 3D MPR plane.
4.Opening the clip arms, adjusting orientation, landing, and closing the clip.
5.Right coronary angiography confirming no impact on the RCA after clipping.
6.Repeating the process for the second clip: steering, rotating, targeting, and engaging the anchor screw.
7.Opening arms, adjusting orientation, landing, and closing the second clip.
8.Right coronary angiography confirming no impact on the RCA before releasing the second implant.
Surgical effect
Comparison of TR regurgitation severity: reduced from 5+ to 2+
preoperative
postoperative
Annular area reduction: 50%

preoperative

postoperative
Surgical Outcomes
- TR Severity Comparison: Reduced from 5+ to 2+.
- Annulus Area Reduction: Decreased by 50%.
- Immediate Overall Verification: At the conclusion of the surgery,复查 (re-examination) via TEE confirmed no residual shunt or pericardial effusion around the LAA occluder, and the tricuspid valve repair results were satisfactory. The patient remained hemodynamically stable, marking the complete success of the one-stop procedure.
Conclusion
The success of this surgery holds value far beyond the technical achievement; it represents a more advanced therapeutic philosophy:
- From "Divide and Conquer" to "Synergistic Governance": Demonstrates the superiority of the multidisciplinary collaboration model within the Cardiovascular Hospital, embodying the modern medical concept of being patient-centric and pursuing maximum clinical benefit.
- From "Minimally Invasive Operation" to "Global Management": Shows that the team possesses not only high-difficulty operational skills but also a global vision, capable of proactively designing optimal treatment pathways for complex patients.
- "Multiplication Effect" of Technology Platforms: The successful combination of K-Clip® and LAAC proves the immense synergistic potential between different device platforms, paving the way for exploring more combined procedural techniques in the future.
Looking ahead, this one-stop combined interventional model, based on "Heart Team" decision-making, is poised to become a crucial direction for managing complex cardiac cases with co-existing conditions. It will enable more patients to welcome a higher quality of life through a single, gentle "heart repair."
Expert Profiles

Liu Jinping
Zhongnan Hospital of Wuhan University

Lu Zhibing
Zhongnan Hospital of Wuhan University

Zhang Gangcheng
Zhongnan Hospital of Wuhan University

Wang Bin
Zhongnan Hospital of Wuhan University

About the K-Clip® Transcatheter Tricuspid Annuloplasty System:
- Minimally Invasive Access: Transvascular puncture approach with minimal trauma; outer sheath diameter is only 18Fr.
- Ease of Use: All operations are performed on the atrial side, featuring a short learning curve.
- Controllability: All steps are reversible before detachment, ensuring controlled surgical outcomes.
Physiological Technology: Achieves annular reduction without damaging native valve leaflets.