First Batch Nationwide | K Clip® Precise Annular Reduction Renews Cardiac Function.Marking a New Era in Tricuspid Valve Interventional Therapy in Shihezi, Xinjiang
Recently, the team led by Professor Guibao He from the Department of Cardiothoracic Surgery at the First Affiliated Hospital of Shihezi University School of Medicine successfully applied the K-Clip® transcatheter tricuspid valve annuloplasty system to perform the first transcatheter tricuspid valve repair procedure in the XPCC (Xinjiang Production and Construction Corps). This breakthrough not only fills the gap in minimally invasive cardiac technology within the XPCC and provides a new minimally invasive treatment option for patients with tricuspid regurgitation, but also marks a new milestone in the development of minimally invasive cardiac treatment in the XPCC.


Tricuspid regurgitation is an insidious clinical problem with significant consequences. Far from being a benign process, it is independently associated with reduced quality of life, increased hospital readmission rates, and shortened survival in patients. The improved screening rate for tricuspid regurgitation in Xinjiang will benefit more patients. The team led by Professor Guibao He from the Department of Cardiothoracic Surgery at the First Affiliated Hospital of Shihezi University School of Medicine enables patients to receive convenient medical treatment locally, fills the regional gap in the diagnosis and treatment of tricuspid valve diseases, and lays a solid foundation for the continuous improvement of regional diagnosis and treatment capabilities.
Patient profile
A 72-year-old female patient was admitted to the hospital with intermittent chest tightness and shortness of breath for 1 week, which had worsened over the past 3 days. The patient reported that her symptoms aggravated upon exertion and relieved with rest. Recently, her chest tightness and shortness of breath deteriorated when lying supine at night. Cardiac ultrasound and coronary CTA were performed after admission. Based on comprehensive evaluation of the examination results, the patient was diagnosed with: 1. Valvular heart disease: severe tricuspid regurgitation (4+), New York Heart Association (NYHA) Class II; 2. Mild pulmonary hypertension. Given the patient's advanced age, she was assessed as being at high risk for conventional surgical intervention.
Preoperative Assessment
Echocardiographic Findings:Severe tricuspid regurgitation (4+; average vena contracta width, 12 mm). The regurgitation was predominantly anteroseptal and central, with a small posteroseptal component. During systole, the anterior and septal leaflets protruded slightly into the right atrium, with a protrusion height of 2.6 mm. A 6 mm gap was observed at the anteroseptal and central regions. Tricuspid annular dilatation was present (mean annular diameter, 40 mm), with a prominent gap at the anteroseptal region.
Preoperative anteroseptal regurgitation
Preoperative 3D view of regurgitation
Preoperative TTE: 4-chamber view regurgitation
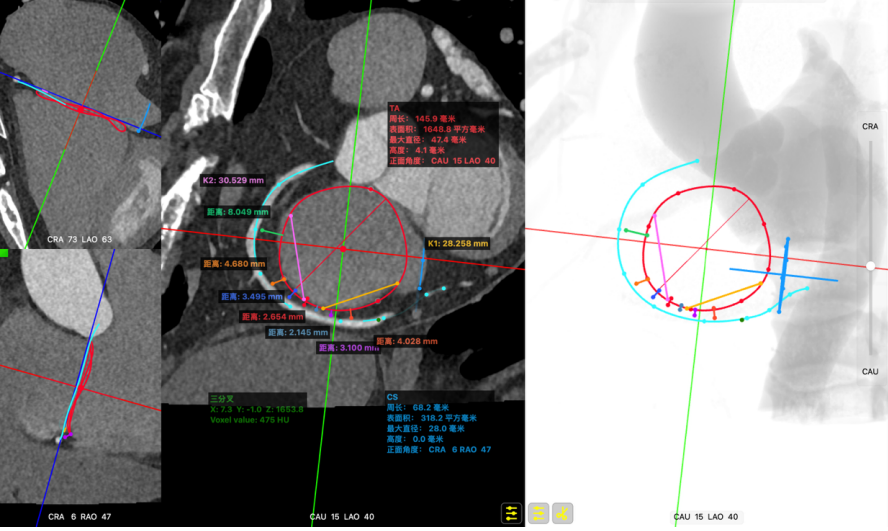
CTA evaluation: Tricuspid annulus dilatation. Diastolic tricuspid annulus circumference: 145.9 mm, area: 1648.8 mm². The right coronary artery (RCA) courses toward the atrial side; the shortest distance between the coronary artery and the annulus during diastole is approximately 2.14 mm, with the RCA deviated to the atrial surface.
Surgical Strategy and Procedure
Professor Guibao He's team developed a personalized treatment plan for the patient based on the patient's anatomical characteristics, disease severity, CTA and echocardiographic findings:
Two K-Clip® devices are planned to be implanted:
Anchor 1: Tricuspid valve short-axis view, 5:00 position, clip model: 14T.
Anchor 2: Tricuspid valve short-axis view, 8:30 position, clip model: 14/16T.
Preoperative simulation predicts regurgitation improvement to grade 2+.
Surgical Procedure
1.Establish a 6F vascular sheath access via the internal jugular vein, withdraw the 6F sheath after inserting a guidewire, then implant an 18F delivery sheath, and secure it to the operating table using a sterile stent base.
2.Under real-time guidance of transesophageal echocardiography (TEE), advance the delivery system into the right atrium and accurately position it at the septal commissure.
The delivery system reaches the right atrium.
Aligned with the posterior septal commissure.
3. Adjust the orientation of the trajectory and drive in the anchoring screw.
Test the trajectory
4. Gently pull the operating lever of the anchoring component to confirm the status of the anchored tissue.
Pull test after anchoring
5. Open the clip device under MultiVue mode, adjust the orientation of the clipping system to be perpendicular to the annulus
Open the clamp after anchoring
6. Switch to MultiVue mode and slowly align the clamping system to the annulus plane.
First device positioned against the annulus
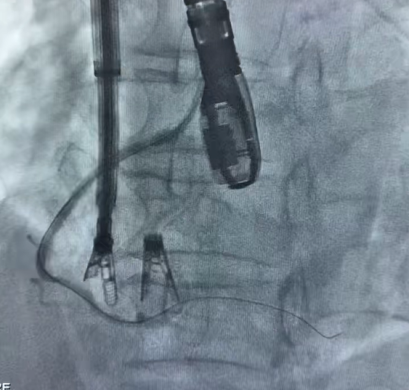
7. Under MultiVue and DSA visualization, pull the anchoring component down to the bottom and close the clamping component.
Observe the closure of the clamp
8. Repeat the above steps for the second clamping component: clamp and deploy it at the annulus in the commissural region between the anterior and posterior leaflets.
The second device is three-dimensionally aligned to the anteroposterior commissure
Second device: adjust trajectory and anchor
The second device is positioned against the annulus
Close the clamp for the second device
9. Postoperatively, evaluate the overall morphology and position of the clipped components using DSA.
Postoperative effect
Comparison of preoperative reflux and postoperative reflux
Preoperative
Preoperative reflux
Preoperative reflux
Postoperative
Postoperative reflux
Postoperative reflux
Immediate Postoperative Echocardiographic Assessment: Tricuspid regurgitation was reduced from preoperative grade 4+ to grade 1+, the annulus diameter was reduced to 6.15 cm², and the leaflet coaptation was satisfactory.
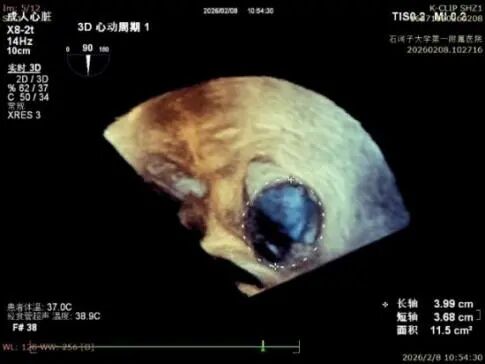
Preoperative annulus area: 11.5 cm²
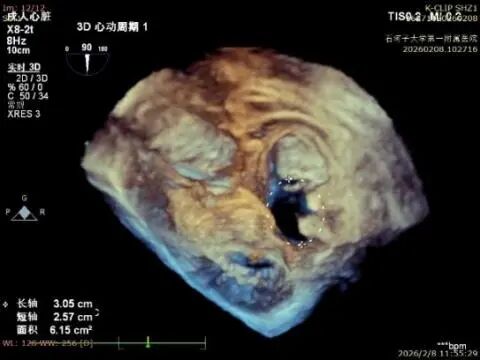
Postoperative annulus area: 6.15 cm²
Group photo after the operation

Expert Comment
Professor He Guibao: Technological innovation empowers clinical practice and tackles the challenges of refractory valvular heart disease.
This patient represents a typical high-risk and complex case of tricuspid regurgitation, for which traditional treatment approaches are limited. With its minimally invasive and precise advantages, K-Clip® has successfully achieved effective annuloplasty of the tricuspid annulus, significantly reducing regurgitation. It features straightforward operation and a short learning curve, while effectively avoiding risks to critical structures such as the coronary arteries. It is expected to become a mainstream option for the treatment of tricuspid regurgitation in the future. The success of this first-in-case procedure not only validates the safety and efficacy of K-Clip® in complex cases, but also marks a key milestone for our region in the field of interventional structural heart disease, enabling more local patients to benefit from domestic innovative medical technologies.
With the promotion of K-Clip®, its clinical application in multiple centers across the country has continued to accumulate extensive experience. It has not only filled the gap in domestic interventional therapy for tricuspid regurgitation, but also stepped onto the international stage as an original Chinese technology. The successful implementation of the first batch of procedures at the First Affiliated Hospital of the School of Medicine, Shihezi University has further expanded the application boundaries of this technology in specific populations, providing a safer and more effective treatment option for patients with tricuspid regurgitation in the region.
In the future, with the widespread adoption of the technology and the accumulation of long-term follow-up data, K-Clip® will continue to address clinical challenges in tricuspid valve treatment, allowing more high-risk patients to overcome the fear of open-heart surgery and regain cardiac vitality!
Expert Profile

He Guibao
The First Affiliated Hospital of the Medical School, Shihezi University

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1.Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2.Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3.All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4.Physiological annuloplasty technology that preserves the native valve leaflets without damage.