Nationwide First Case | Shandong Provincial Hospital Affiliated to Shandong First Medical University Adopts K-Clip® for Precise Treatment of Severe Tricuspid Regurgitation
Recently, the Department of Cardiac and Macrovascular Surgery of Shandong Provincial Hospital Affiliated to Shandong First Medical University (Shandong Provincial Hospital), led by Professor Wang Anbiao, together with Professor Dong Mingliang from the Department of Cardiac Surgery, and multidisciplinary teams including the Department of Cardiac Ultrasound, Anesthesiology and Operating Room, has successfully completed the clinical application of the K-Clip® Transcatheter Tricuspid Valve Annuloplasty System. The medical team performed transcatheter tricuspid interventional in a patient with severe tricuspid regurgitation,achieving minimally invasive and precise treatment. After the operation, the patient’s tricuspid regurgitation was significantly relieved with favorable recovery, and the patient has been discharged from hospital upon full recovery.

Patient's Profile
History of Present Illness: One month ago, the patient developed chest tightness and shortness of breath without obvious inducement. There was no chest pain, palpitations, cough, sputum production, nausea or vomiting. The patient subsequently visited a local hospital for treatment, where echocardiography revealed “post‑mitral mechanical valve replacement, tricuspid regurgitation.”The patient was referred to a higher-level hospital for further management. Later, the patient presented to Shandong Provincial Hospital Affiliated to Shandong First Medical University. Outpatient cardiac ultrasound indicated: post-mitral valve replacement, severe tricuspid regurgitation, ultrasonic manifestations of cardiac insufficiency, and pulmonary hypertension. Surgical intervention was therefore recommended. After consultation by the Department of Cardiac and Great Vascular Surgery, surgical treatment for tricuspid valve disease was advised. To balance therapeutic efficacy and procedural safety, a multidisciplinary discussion was conducted. The medical team ultimately decided to perform transcatheter tricuspid annuloplasty, which features minimal trauma, rapid recovery, definite clinical efficacy and high safety profile.
Preoperative Evaluation
Echocardiography indicated: severe tricuspid regurgitation and postoperative mitral valve replacement.
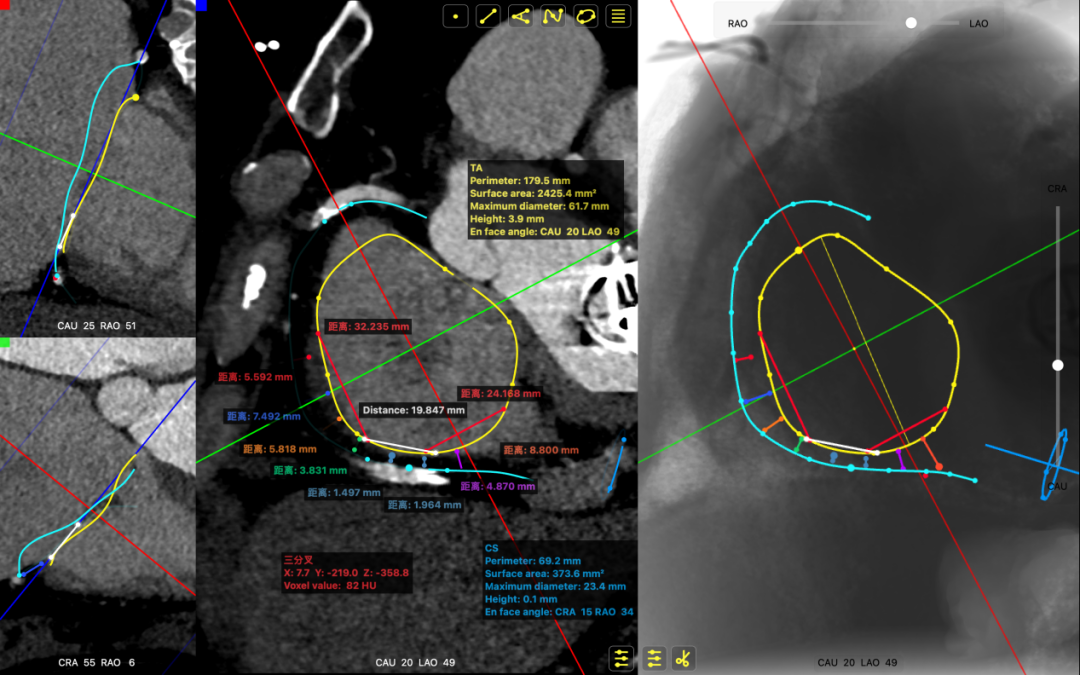
CTA findings: Cir: 179.5 mm, Area: 2425.4 mm².
Surgical Strategy
The patient suffered from functional tricuspid regurgitation complicated with multiple comorbidities including atrial fibrillation, with a clear surgical indication. After comprehensive evaluation by the cardiac team, transcatheter tricuspid annuloplasty was planned. Based on preoperative assessment, 14T and 16T K‑Clip® clamping devices were to be implanted at the posterior annulus and anteroposterior annulus respectively. This strategy could reduce the circumferential length and area of the tricuspid annulus, improve leaflet coaptation, and ultimately alleviate tricuspid regurgitation.
Intraoperative Procedure

Under general anesthesia, jugular vein puncture was performed to establish the access. An 18Fr steerable delivery sheath was advanced to the middle and lower segment of the right atrium over a stiff guidewire. Under echocardiographic guidance, the delivery system was delivered, and 14T and 16T K‑Clip® devices were implanted at the posterior tricuspid annulus and anteroposterior annulus respectively. The angle between the device and the annular plane was adjusted by bending and rotation to direct the tip of the clip toward the target lesion. With the assistance of echocardiographic MPR mode, the anchoring components were deployed at the annulus. After traction and stabilization, the clamping arms were opened and closely attached to the annular tissue. Subsequently, the anchoring components were retracted to close the clamping arms and accomplish annular reduction. Satisfactory procedural outcome was confirmed by intraoperative evaluation, and the clip devices were finally released.
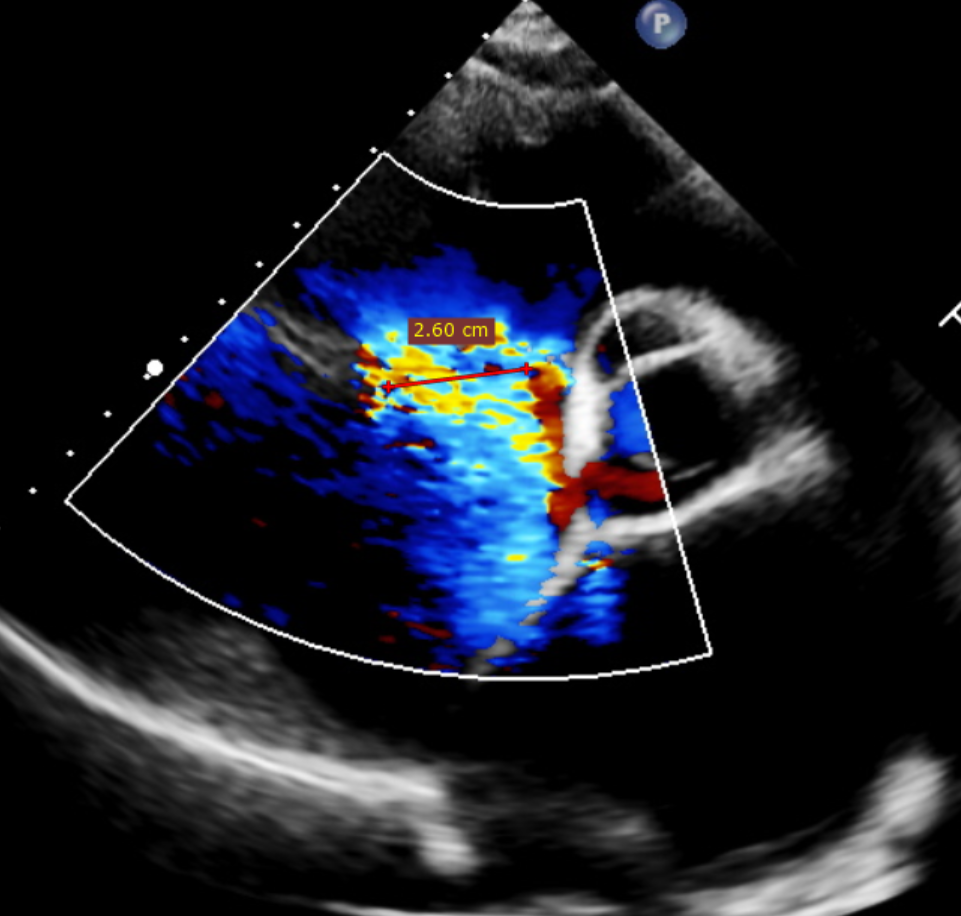
1.Preoperative Regurgitation and RCA Angiography
Preoperative Tricuspid Regurgitation

Preoperative Coronary Angiography
2. First Clipping of Posterior Annulus Region
Clipped Septal Region
First clipping: RCA blood flow
3. Second Clipping of the Anteroposterior Annulus Region
Second clipping of the anteroseptal and posterior region
Second patency of blood flow
Procedural Outcome
After implantation of two K-Clip® devices (14T and 16T) at the posterior and anteroposterior tricuspid annulus, the tricuspid annular area decreased from 21.9 cm² preoperatively to 11.5 cm². Tricuspid leaflet coaptation was significantly improved. The degree of regurgitation was reduced from grade 5+ to grade 2+. The overall procedural outcome met expectations, and the operation was completed successfully.
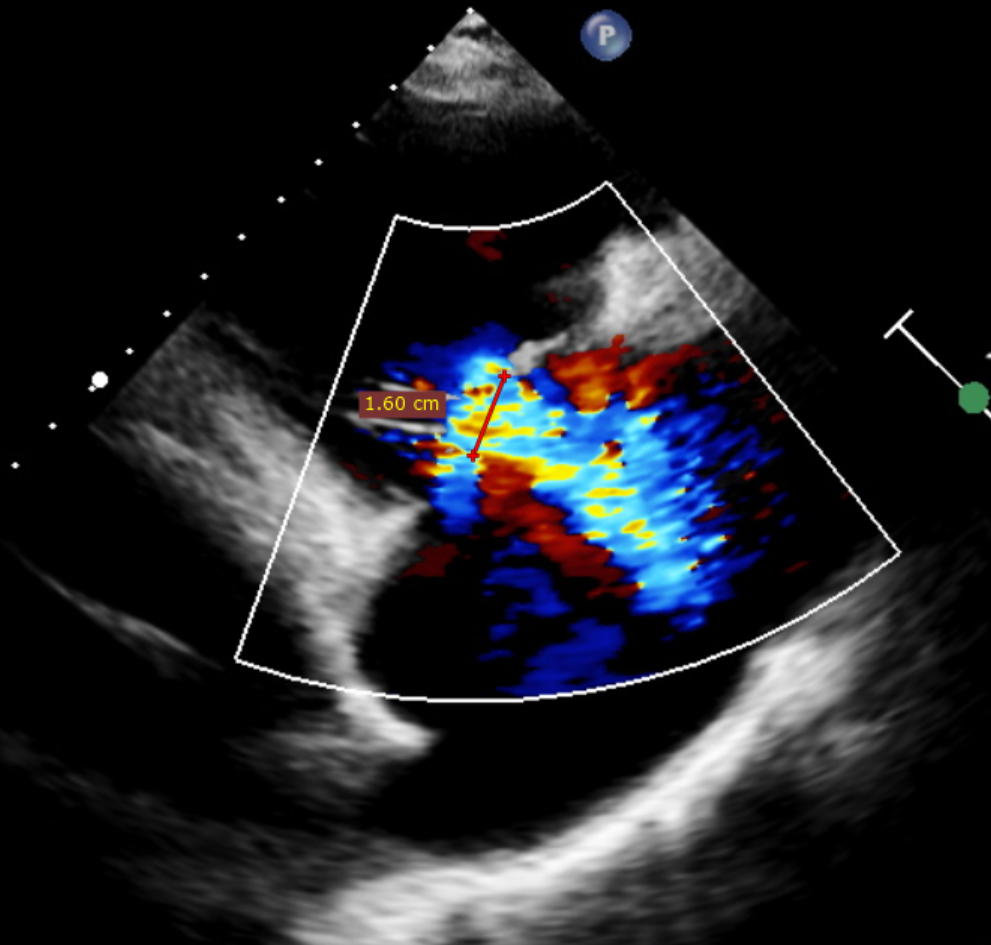
Postoperative Regurgitation Comparison
Procedural Outcome: The tricuspid regurgitation was reduced from severe grade 5+ to mild-to-moderate grade 2+.
Preoperative tricuspid regurgitation
Postoperative Regurgitation
Valvular heart disease is a common severe cardiovascular disorder in clinical practice. Mitral valve replacement, as a classic surgical procedure for severe mitral valve lesions, has been widely applied clinically and has saved numerous patients’ lives. However, in clinical practice, some patients may develop secondary tricuspid annular dilatation and poor leaflet coaptation after surgery, which further progresses to severe or even massive tricuspid regurgitation. Such secondary lesions are often accompanied by a series of complications including progressive deterioration of right ventricular function, systemic congestion and refractory heart failure. These conditions seriously impair patients’ quality of life and threaten their life safety, remaining a challenging problem to be urgently addressed in the field of cardiovascular diagnosis and treatment.
Compared with primary tricuspid valve disease, patients with massive tricuspid regurgitation secondary to mitral valve replacement usually have a history of previous thoracotomy, impaired cardiopulmonary function, and combined multisystem underlying diseases. These factors lead to an extremely high risk of repeat open-heart surgery, with markedly increased perioperative mortality and complication rates. Conventional medical conservative treatment is insufficient to reverse structural abnormalities of the valve leaflets or halt the progression of regurgitation, resulting in a poor long‑term prognosis. Therefore, safe, effective and minimally invasive therapeutic alternatives are urgently needed in clinical practice to address this therapeutic dilemma.
In recent years, the rapid advancement of transcatheter valve intervention technology has provided novel therapeutic options for high-risk patients with severe valvular heart disease. As an innovative minimally invasive interventional device, the K‑Clip® transcatheter tricuspid annuloplasty system possesses core advantages including a minimally invasive transjugular approach, physiological annular reduction, preservation of native valve leaflets, and reversible and controllable procedural characteristics, offering a new strategy for the management of massive tricuspid regurgitation. This technique accurately replicates the principle of classic surgical procedures. It plicates the dilated tricuspid annulus via an interventional approach, reduces annular circumference, improves leaflet coaptation, and effectively relieves regurgitation. It balances therapeutic efficacy and procedural safety, and is particularly suitable for critically ill complex patients with high surgical risk or surgical contraindications.
Summary
As a top-tier comprehensive Grade A tertiary hospital in the region, Shandong Provincial Hospital has long been committed to the diagnosis and treatment of complex and severe cardiovascular diseases in the Department of Cardiac and Macrovascular Surgery, continuously tackling difficult and complicated cases and optimizing minimally invasive diagnosis and treatment technologies. In this procedure, the cardiovascular surgery team of the hospital overcame multiple challenges and successfully performed transcatheter intervention with the K-Clip® system for a patient with massive tricuspid regurgitation secondary to mitral valve replacement. This intervention not only breaks through the treatment bottleneck for such high-risk and complex cases and fills the regional gap in the application of relevant minimally invasive techniques, but also demonstrates the hospital’s solid strength and innovative capacity in the interventional diagnosis and treatment of structural heart disease. The successful completion of this surgery has accumulated valuable clinical experience for the standardized and minimally invasive management of severe secondary tricuspid regurgitation after mitral valve surgery. It also brings higher-quality and more precise treatment prospects for a large number of high-risk patients with valvular heart disease, and strongly promotes the high-quality development of regional cardiovascular interventional medicine.
Expert Introduction

Wang Anbiao
Shandong Provincial Hospital Affiliated to Shandong First Medical University

Dong Mingliang
Shandong Provincial Hospital Affiliated to Shandong First Medical University

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1.Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2.Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3.All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4.Physiological annuloplasty technology that preserves the native valve leaflets without damage.