Successful Completion of a "One-Stop" K-Clip® Combined with M-TEER Procedure at Sun Yat-sen Memorial Hospital of Sun Yat-sen University
Recently, led by President Chen Yangxin and Professor Zhou Shuxian, the heart valve team of Sun Yat-sen Memorial Hospital, Sun Yat-sen University, with the seamless collaboration of the Department of Ultrasound, Catheterization Laboratory, Department of Anesthesiology and nursing team, has successfully performed a one-stop procedure for a patient with severe global heart failure complicated by complex severe mitral regurgitation (MR) and torrential tricuspid regurgitation (TR). As a national demonstration base for innovative medical technologies, Sun Yat-sen Memorial Hospital, Sun Yat-sen University continuously explores the efficacy and feasibility of novel therapeutic regimens, aiming to provide more treatment options for patients.

The patient presented with severe functional mitral regurgitation and torrential tricuspid insufficiency. Transesophageal echocardiography (TEE) assessment confirmed that the mitral valve anatomy was suitable for transcatheter mitral edge-to-edge repair (M-TEER). However, the patient had marked tricuspid annular dilatation with significantly widened inter-valvular gaps, making transcatheter tricuspid edge-to-edge repair (T-TEER) inappropriate. After thorough multidisciplinary team (MDT) discussion and full consideration of the patient’s preference, the heart team decided to perform transcatheter tricuspid annular repair (K-Clip®) combined with simultaneous transcatheter mitral edge-to-edge repair (MitraClip-TEER). The one-stop procedure successfully corrected both mitral regurgitation and tricuspid regurgitation in a single session.
Preoperative Evaluation of Mitral Valve
Severe functional mitral regurgitation (FMR, grade 4+).P2 length: 18 mm, A2 length: 26 mm, AP diameter: 37 mm. Sufficient mitral orifice area; interatrial septum height: 4.5 cm.
Preoperative 3D
Preoperative 2D color Doppler
Preoperative 3D color Doppler
The Procedure of TEER Surgery
After thorough analysis and discussion of the case by Professor Chen Yangxin’s team, considering the adequate length of the posterior mitral leaflet, excessively wide regurgitant jet, and mildly enlarged anteroposterior annular diameter, the team finally decided to implant two XTR clips at segment 2 where regurgitation was most severe. This strategy not only effectively reduced regurgitation but also distributed tension across the two clips, lowering the risk of leaflet tear.
Transseptal puncture
Guide sheath advanced into the left atrium
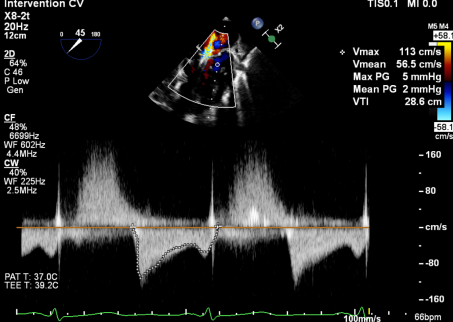
After deployment of the first XTR clip, mitral regurgitation was significantly reduced, with residual regurgitation predominantly located laterally. The mean transvalvular pressure gradient was 2 mmHg. Therefore, a second XTR clip was implanted side-by-side at the lateral aspect.
Implantation Procedure of the First Clip:
Implantation Procedure of the Second Clip:
After full release of the clip, regurgitation was reduced to mild-to-moderate, with stable clip configuration.
Tricuspid Valve Preoperative Evaluation
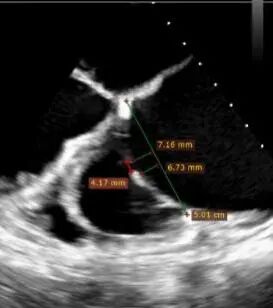
Echocardiographic findings: Severe torrential tricuspid regurgitation (grade 5+, average vena contracta width: 14 mm) with tricuspid annular dilatation (mean annular diameter: 42 mm). Regurgitant orifices were located at the anteroseptal, central, anteroposterior and posteroseptal regions. Remarkable gaps were noted between each tricuspid leaflet segments: Anteroseptal gap: 4.1 mm, Anteroposterior gap: 6.6 mm, Posteroseptal gap: 7 mm, Central gap: 10 × 6 mm, Total gap area: 1.79 cm².


CTA Examination and Surgical Strategy
Annular area: 17.2 cm² (severe dilatation). The distance between the RCA and tricuspid annulus (TA) remained over 3 mm throughout the entire cardiac cycle, with a minimum distance of 5 mm, indicating low coronary artery risk.
Combined with comprehensive preoperative evaluation by CT and TEE, the patient presented with severe tricuspid annular dilatation and extensive gaps at both the commissures and central region. Regurgitation originated mainly from the posteroseptal central and anteroseptal segments. The procedure was considered technically challenging. It was planned to deploy 14T K‑Clip® devices at the posteroseptal commissure and anteroposterior commissure respectively. This strategy aims to reduce the tricuspid annular circumference and enlarge the leaflet coaptation margin, thereby alleviating tricuspid regurgitation.

K-Clip® Procedural Process

After general anesthesia, internal jugular vein puncture was performed to establish vascular access, and one Proglide device was pre-deployed. An 18Fr delivery sheath was advanced over a stiff guidewire to the mid-right atrium. Under ultrasound guidance, the delivery system was inserted. Two 14T K-Clip® devices were deployed at the posteroseptal commissure and anteroposterior commissure respectively. The angulation between the device and the annular plane was adjusted by curve control and rotation to direct the tip of the clip toward the target site. Under ultrasound MPR mode, the anchoring component was anchored at the tricuspid annulus. After traction and stabilization, the grasping arms were opened and apposed to the annulus. Subsequently, the anchoring component was retracted to close the grasping arms and achieve annular plication. With satisfactory procedural effect confirmed, the clip assembly was released and detached.
The delivery system was advanced into the right atrium via the superior vena cava (SVC).
Adjust the delivery system toward the target site.
Under MPR view, the anchoring component was anchored into place.
Open the grasping arms, adjust the orientation, and then appose to the annulus.
Close the grasping arms to reduce the annular circumference.
Advance the second clip into position.
Determine screw penetration into the hinge point under MPR view.
Confirm the orientation of the second clip.
Close the second clip.
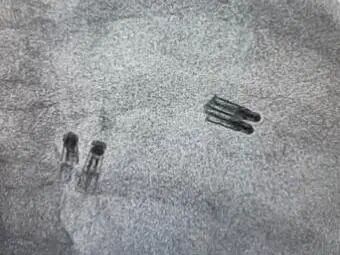
DSA morphology after detachment of two K‑Clip® devices and two XTR devices
Procedural outcome
After one 14T K‑Clip® was implanted at the annular commissure between the posterior and septal leaflets of the tricuspid valve, another 14T K‑Clip® was subsequently deployed at the annular commissure between the posterior and anterior leaflets. The overall tricuspid annular area decreased by 36%. The central inter-leaflet gap was significantly reduced, and leaflet coaptation was markedly improved. Tricuspid regurgitation was downgraded from preoperative torrential severity to mild-to-moderate grade. The overall procedural outcome exceeded expectations, and the operation was completed successfully.
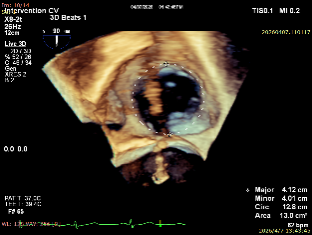
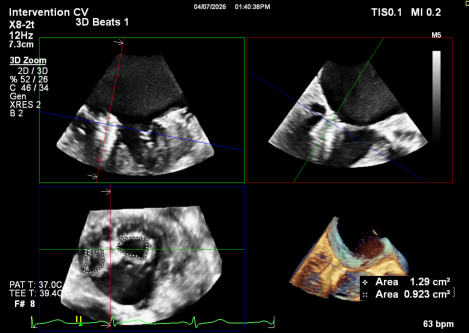
Preoperative annular area: 13 cm²
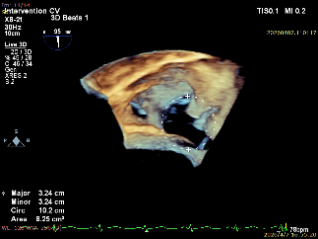
After deployment of two clips, the tricuspid annular area was 8.25 cm².
Preoperative regurgitation in the gastric fundus view
Postoperative regurgitation in the gastric fundus view
Expert Introduction

Chen Yangxin
Sun Yat-sen Memorial Hospital, Sun Yat-sen University
Deng Bingqing
Sun Yat-sen Memorial Hospital, Sun Yat-sen University

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1.Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2.Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3.All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4.Physiological annuloplasty technology that preserves the native valve leaflets without damage.