Among the first nationwide! The Cardiology Team of Shanghai Changhai Hospital has successfully performed the first K Clip® procedure for patients with severe tricuspid regurgitation!
Recently, led by Professor Zhifu Guo and the team of Professor Yuan Bai from the Department of Cardiology, Changhai Hospital of Shanghai, the K‑Clip® Transcatheter Tricuspid Annuloplasty System was successfully applied to treat a patient with severe tricuspid regurgitation. Previously, the patient had undergone transcatheter mitral edge‑to‑edge repair for severe mitral regurgitation at the same hospital. More than two years after the procedure, symptoms of heart failure recurred, with severe tricuspid regurgitation identified as the underlying cause. Adopting K‑Clip® transcatheter tricuspid annuloplasty, one of China’s most advanced cutting‑edge interventional cardiology technologies, the cardiology team only implanted two clip devices via jugular vein puncture. The tricuspid regurgitation was reduced from severe (4+) to mild (1+). The surgery was safe with definitive efficacy, significantly improving the patient’s quality of life.


Patient Profile
The patient is male.
Chief Complaint: Fatigue in limbs and dyspnea after physical exertion for over 10 years, aggravated for 2 months.
History of Present Illness: Around 2015, the patient developed exertional dyspnea without obvious inducement, which could be relieved by rest. In December 2017, his symptoms worsened, accompanied by recurrent low‑grade fever and dyspnea. He sought medical care at a local hospital, where echocardiography revealed a left ventricular aneurysm. He subsequently underwent ventricular aneurysm resection in the Department of Cardiac Surgery at Changhai Hospital of Shanghai. His symptoms temporarily resolved after surgery, but recurred in 2019. He was admitted for further treatment and diagnosed with severe mitral regurgitation and pulmonary hypertension. Despite standardized pharmacological therapy for heart failure, his symptoms persisted. On December 28, 2023, he received transcatheter mitral edge‑to‑edge repair (TEER) at the same hospital. Postoperatively, his chest tightness was significantly alleviated, and follow‑up echocardiography showed markedly reduced regurgitation volume. In early February 2026, the patient developed recurrent symptoms with lower‑extremity and facial edema. He presented to this hospital for treatment and was admitted under the outpatient diagnosis of tricuspid regurgitation.
Diagnoses upon admission: 1. Severe tricuspid regurgitation. 2. Status post mitral edge‑to‑edge repair. 3. Chronic heart failure. 4. Pulmonary hypertension.
Preoperative Evaluation
Echocardiography findings: Post‑M‑TEER status, severe tricuspid regurgitation (4+, mean vena contracta: 10 mm), with regurgitant orifice located at the posteroseptal and central regions. Mild tricuspid annular dilatation (mean annular diameter: 41 mm). No obvious leaflet tethering or gaps were observed.
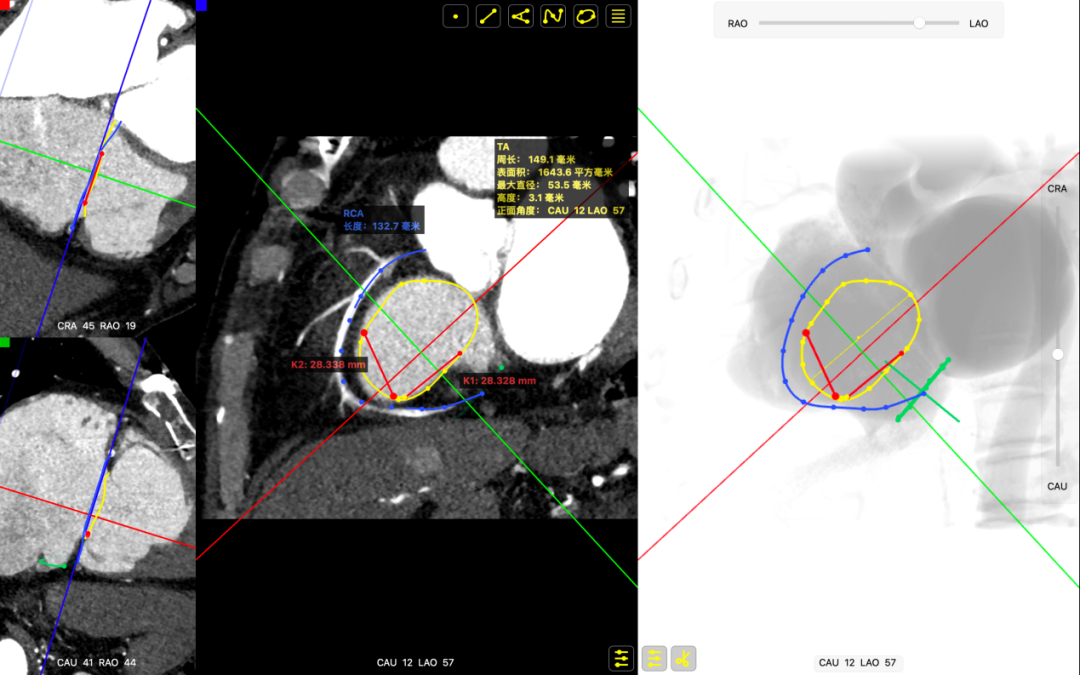
CTA findings: Circumference (Cir): 149.1 mm, Area: 1643.6 mm².
Surgical Strategy
Based on comprehensive preoperative evaluation of CT and echocardiography, this patient presented with mild tricuspid annular dilatation and regurgitation mainly originating from the anteroseptal and central regions, with clear surgical indications. After multidisciplinary assessment by the cardiology team, transcatheter tricuspid annuloplasty was planned. Two clip devices, 14T K‑Clip® and 12T K‑Clip®, were intended to be deployed at the posterior annulus to reduce annular circumference and improve leaflet coaptation, thereby alleviating tricuspid regurgitation.
Operative Procedure
After general anesthesia, jugular vein puncture was performed to establish vascular access. An 18‑Fr delivery sheath was advanced to the mid‑right atrium over a stiff guidewire. Under ultrasound guidance, the delivery system was deployed, with the 14T K‑Clip® and 12T K‑Clip® clip devices implanted at the posterior tricuspid annulus respectively. Angular alignment between the device and the annular plane was adjusted by deflection and rotation to direct the tip of the clip devices toward the target site. Under ultrasound MPR mode, anchoring components were deployed at the annulus. After stabilization via traction, the grasping arms were opened and apposed to the annulus. The anchoring components were then retracted to close the grasping arms for annular plication. Satisfactory procedural outcomes were confirmed, and the clip delivery components were released.
The delivery system enters the right atrium (RA) via the superior vena cava (SVC).
Adjust the delivery system to target the lesion site.
Deploy the anchoring component under the MPR view.
Open the grasping arms, adjust the orientation, and appose them to the annulus.
Close the grasping arms to reduce the annular size.
Deploy the second clip.
Screw penetration into the hinge point confirmed under MPR view
Confirm the orientation of the second clip
Close the second clip.

DSA angiography confirmed grade 3 coronary blood flow.
Procedural Outcome
The overall tricuspid annular area decreased by 45%, leaflet coaptation improved, and regurgitation was significantly reduced from severe (4+) pre‑operatively to mild (1+). The overall procedural outcome exceeded expectations, and the surgery was successfully completed.
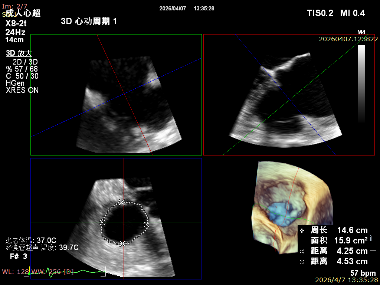
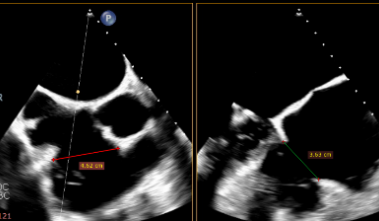
Preoperative tricuspid annular area: 15.9 cm²
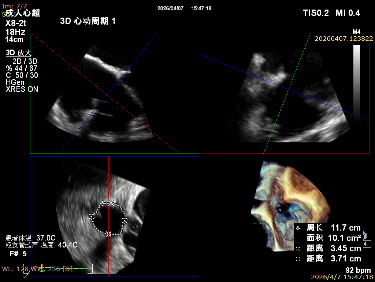
The tricuspid annular area was 10.1 cm² after deployment of two clips.
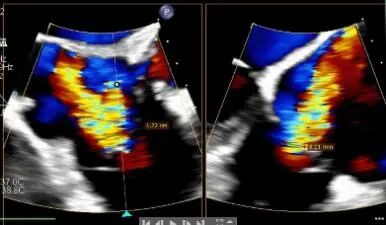
Baseline regurgitation after anesthesia
Postoperative regurgitation
Summary
This procedure was performed by the team led by Professors Guo Zhifu and Bai Yuan from the Department of Cardiology of Changhai Hospital. As one of the first national experts in K‑Clip® implantation, the team conducted tricuspid annuloplasty and mitral valve repair, both of which are cutting‑edge interventional cardiology techniques. This marks a leap in cardiac valve technology from open‑heart surgery to minimally invasive intervention. The successful K‑Clip® procedure signifies another milestone for Changhai Hospital in Shanghai in the field of interventional treatment for valvular heart disease, bringing new hope to more critically ill patients with tricuspid regurgitation.
Expert Profile

Guo Zhifu
The First Affiliated Hospital of Naval Medical University (Shanghai Changhai Hospital)

Bai Yuan
The First Affiliated Hospital of Naval Medical University (Shanghai Changhai Hospital)

Zhu Jiaqi
The First Affiliated Hospital of Naval Medical University (Shanghai Changhai Hospital)

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1.Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2.Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3.All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4.Physiological annuloplasty technology that preserves the native valve leaflets without damage.